
Executive summary
Analyze Consulting was approached by a hospital trust to assist in improving process efficiency at a South African tertiary hospital. The trust works closely with the hospital by providing funding for projects. The hospital hoped to improve the quality of service delivery throughout its clinics by applying practical, cost-effective solutions to problem areas.
To achieve this, Analyze Consulting assisted them in identifying major areas of inefficiency, the root causes of these inefficiencies and solutions for improvement. Valuable insights were revealed through data collection in the form of surveys and interviews which provided management with focus areas for improvement.

Background
In South Africa, demand, under-funding and insufficient human resources are the three major challenges facing the public healthcare sector. Approximately 83.1% of South Africans do not have medical aid, and the total spent on non-medical aid patients is approximately 15% of the total healthcare budget. Budget cuts have become a daily challenge facing those working in public healthcare. Therefore, hospitals have had to find creative and cost-effective solutions that add the most value with their current resources.
Challenges
Budget cuts in the South African public healthcare sector have forced hospitals to reduce their expenditure. In many cases, this has led to issues such as the following observed in the general outpatient clinic:
Budget cuts have become a daily challenge facing those working in public healthcare. Therefore, hospitals have had to find creative and cost-effective solutions that add the most value.
* The average number of patients being booked is 11% more than the average number of patients that can be treated. This results in patients having to wait longer to be treated as staff have a greater backlog of patients.
* 22% of treated patients are walk-ins (patients with no bookings). This adds extra admin responsibilities for staff, i.e. preparing unexpected patient folders which take time away from staff caring for patients.
* 29% of booked patients are not arriving for their appointments. Staff spend a copious amount of time preparing for these patients. This time could be utilised elsewhere.
* 29% of patients are arriving without the required documentation. This results in the hospital not having up-to-date patient information which leads to billing and contact issues. Clerks currently inform patients about required documents while they are making a booking, or nurses will inform patients before the clinic begins. However, this strategy is not effective in reducing the number of patients that are arriving without required documentation.
* Patients are waiting an average of three hours and 15 minutes to be treated, compared to the South African tertiary hospital average of four hours. Although waiting time is less than the national average, the hospital's objective is to reduce this waiting time even further.
* Staff feel demotivated as they are overburdened with additional admin responsibilities due to excessive booking numbers.
Approach to gather insights
1. Selection: Analyze Consulting started by selecting a focus area in the hospital that was flagged for major inefficiencies. Various clinics were recommended by management, and the general outpatient clinic was one of two clinics which were selected by the Analyze Consulting team.
2. Observation and data collection: Patients were observed on their journeys in and around the general outpatient clinic. Waiting times, interactions between staff and other areas of the hospital and the patient's experience and morale throughout their journey was noted. The Analyze Consulting team followed each patient on their journey from the point that they arrived at the hospital until they left.
Throughout the patient's journey, they were asked about their satisfaction and mood. Observing the patient's journey provided valuable insights; waiting times, patient experience, patient background information and feedback/improvement suggestions. The problem, however, was that the patient journey observations did not reveal problems that were occurring outside of the patient's journey, i.e. problems inside the hospital. To highlight these internal issues and their severity, interviews were conducted with patients and staff, and surveys were sent out to collect data.
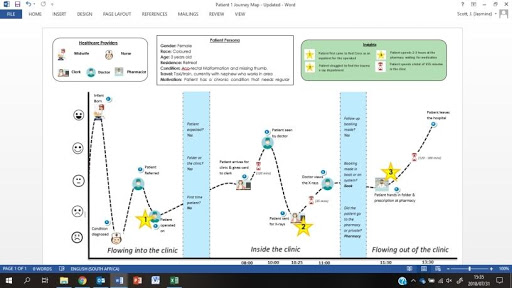
3. Analysis and documentation: Patient journeys were documented in patient journey maps (illustrated below) and then analysed. Survey data was recorded in Excel and graphs were generated to provide a quick and visual overview of problem areas. Issues, root causes and recommendations were documented.
4. Results and proposal: Patient journey maps, issues, root causes and recommendations were presented to management. Discussions were formed around practical solutions that could improve internal issues.
How Analyze helped
The project involved both quantitative and qualitative data gathering in the form of surveys and interviews. The survey asked for details about patient waiting times, staff/patient experience, required documentation and patient folder information.
The data was then analysed, and the main challenges were highlighted. The data showed that a lack of control of bookings from referral and internal networks and the high number of bookings being made contributed greatly to service delivery. Additionally, interviews with staff highlighted that many patients and staff members were not following the correct booking procedure. The Analyze Consulting team suggested that as part of the solution rollout, staff should be educated on the correct booking procedure and be rewarded/incentivised to sustain this behaviour.
The Analyze Consulting team recommended that booking numbers per clinic be capped at 50 booked patients. If booked patients are capped at 50, data and calculations have shown that patients will wait for a total of two hours and nine minutes on average. Patients are currently waiting for a total of three hours and 15 minutes on average. This will be a 34% improvement in total waiting time.
Extensive clinic planning was discussed with management to ensure that this patient limit can be seamlessly implemented. The details of this plan, as well as the required information that needs to be fed into the clinic, were discussed with management in various meetings and presentations. The Analyze Consulting team recommended that continuous data collection be employed as part of the staffs' daily activities in order to keep track of the effectiveness of the implemented solution.
Future plans
Instead of implementing big changes within the clinic in one go, management's goal is to start small and incrementally control bookings coming into the clinic. If there is effective control on bookings flowing into the clinic, it will help to improve other problem areas that stem from booking inefficiency. Management is now looking at other potential areas where they can apply these insights and solutions to.
Share